The neck hides a surprisingly busy patch of anatomy just below the jaw. This small area holds glands, vessels, nerves, and lymph nodes that work together every day, often without notice. Doctors, dentists, and students study this zone closely because problems here can affect swallowing, speech, and even breathing. In this guide, we explore the submandibular region step by step, covering its borders, its contents, and why it matters in real clinical practice. Along the way, we break down each structure so you can picture exactly what sits where.
Understanding this area builds a strong foundation for head and neck anatomy. Therefore, we keep the explanations simple and visual, using tables and a flowchart to make the layout easy to remember.
Boundaries of the Submandibular Region
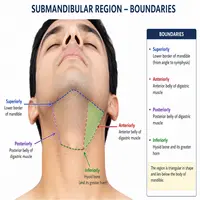
Every anatomical space needs clear borders, and this one is no exception. The area sits within the digastric triangle, tucked beneath the lower jaw.
Its boundaries include:
- Superiorly: the body of the mandible
- Anteriorly and posteriorly: the two bellies of the digastric muscle
- Roof: skin, superficial fascia, and platysma
- Floor: mylohyoid and hyoglossus muscles
Notably, the mylohyoid muscle splits this space into two smaller compartments. One lies above the muscle, while the other lies below it. This division matters because the submandibular gland actually wraps around the free edge of mylohyoid, occupying both compartments at once.
Additionally, the shape of this triangular space changes slightly with head position. When the neck extends, the boundaries stretch and become easier to palpate during a clinical exam. Consequently, clinicians often ask patients to tilt their head back before checking for swelling or tenderness in this zone.
Structures Within the Submandibular Region
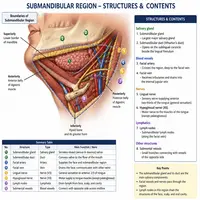
Several important structures crowd into this compact space. Below is a simple table summarizing them.
| Structure | Type | Key Detail |
|---|---|---|
| Submandibular gland | Salivary gland | Largest structure, wraps around mylohyoid |
| Submandibular lymph nodes | Lymphatic | Drain lips, cheeks, and anterior tongue |
| Facial artery | Blood vessel | Grooves the posterior part of the gland |
| Facial vein | Blood vessel | Runs superficial to the gland |
| Hypoglossal nerve | Cranial nerve (CN XII) | Lies deep to the gland, supplies tongue muscles |
| Lingual nerve | Sensory nerve | Loops below the submandibular duct |
| Mylohyoid nerve and vessels | Nerve/vessel | Supply the mylohyoid muscle and floor of mouth |
The gland itself has two parts: a larger superficial lobe and a smaller deep lobe. Meanwhile, its duct, called Wharton’s duct, travels forward to open near the base of the tongue. This duct plays a major role in saliva delivery, so any blockage here often causes noticeable swelling after meals.
Furthermore, the submandibular lymph nodes act as a drainage checkpoint. They collect lymph from the face, gums, and tongue before passing it along to deeper cervical nodes. As a result, doctors frequently examine this area first when investigating oral or facial infections.
Neurovascular Relations Explained
Nerves and vessels travel through this space in a fairly predictable pattern. The flowchart below outlines the basic relationship between the gland, duct, and nearby nerves.
Facial Artery
|
v
Grooves Submandibular Gland (posterior surface)
|
v
Submandibular Duct (Wharton's Duct)
|
v
Crossed twice by the Lingual Nerve
|
v
Opens at the Sublingual PapillaThis crossing pattern is a classic exam topic. The lingual nerve first runs lateral to the duct, then crosses beneath it, and finally lies medial to the duct near the tongue. In contrast, the hypoglossal nerve stays deep to the gland throughout its course and never crosses the duct at all.
Similarly, the marginal mandibular branch of the facial nerve deserves attention, even though it sits just outside the strict boundaries of this space. It runs close to the gland’s superficial surface, which is why surgeons stay cautious during gland removal. Damage to this nerve can cause drooping at the corner of the mouth.
Clinical Significance of the Submandibular Region
Clinicians pay close attention to this region for good reason. Swelling, pain, or lumps here often point toward specific, identifiable problems.
Common conditions include:
- Sialadenitis – inflammation of the submandibular gland, often linked to dehydration or duct blockage.
- Sialolithiasis – stone formation within Wharton’s duct, since its upward course and thick saliva make stones more likely here than in other glands.
- Lymphadenopathy – enlarged lymph nodes from dental infections, tonsillitis, or, less commonly, malignancy.
- Ludwig’s angina – a serious, rapidly spreading infection of the floor of the mouth that can compress the airway.
- Submandibular gland tumors – uncommon, but they require careful evaluation due to nearby nerves.
Because saliva flow depends on gravity and duct anatomy, blockages tend to cause pain that worsens around mealtimes. Patients often describe swelling that rises just before eating and settles down afterward. This pattern alone gives clinicians a strong clue before any imaging takes place.
Moreover, dentists and ENT specialists often collaborate when problems arise in this area. A tooth infection, for instance, can easily spread and irritate the nearby lymph nodes, mimicking a gland problem. Accurate diagnosis, therefore, depends on examining the mouth, teeth, and neck together rather than in isolation.
Diagnostic and Surgical Considerations
Doctors typically start with a physical exam, feeling for masses both inside the mouth and externally along the jawline. Ultrasound often follows, since it detects stones, cysts, and gland enlargement without radiation exposure. In more complex cases, a CT scan or sialography may help map out the duct system clearly.
Surgical removal of the submandibular gland, when necessary, requires careful planning. Surgeons must protect several nearby nerves, including the marginal mandibular, lingual, and hypoglossal nerves. Consequently, this procedure ranks among the more delicate operations in head and neck surgery, despite its relatively small incision.
Recovery generally goes smoothly when nerves remain undamaged. However, temporary numbness of the tongue or a subtle change in smile symmetry can occur if a nerve gets stretched during the procedure. Most of these effects fade within weeks.
Conclusion
The submandibular region may be small, but it carries real clinical weight. From salivary drainage to lymphatic filtering, this compact space plays several roles at once. Its boundaries, muscles, nerves, and vessels fit together in a pattern that rewards careful study. Whether you’re a student preparing for an anatomy exam or a clinician assessing neck swelling, a solid grasp of this area pays off quickly. Keep the table and flowchart above handy, and the relationships here will start to feel far less overwhelming.
Frequently Asked Questions
It sits just below the body of the mandible, within the digastric triangle of the neck, bordered by the two bellies of the digastric muscle.
The submandibular gland is the largest and most clinically important structure here, along with its duct, nearby lymph nodes, and several key nerves.
The lingual nerve crosses the submandibular duct twice, making it an important landmark during gland surgery and a common source of exam questions.
Swelling often comes from duct stones, gland infection, or enlarged lymph nodes reacting to dental or oral infections.
It carries some risk mainly due to nearby nerves, particularly the marginal mandibular and hypoglossal nerves, but experienced surgeons manage this safely in most cases.