The osteology of head and neck decides more BDS results than any other region of the body, and the orbit, the pharyngeal apparatus, and the skull foramina sit right at the centre of that syllabus. Consequently, this guide condenses the most exam-relevant topics from BD Chaurasia’s Human Anatomy into one quick-revision article on the osteology of head and neck. Furthermore, every section below uses tables and a flowchart so that the relationships between structures, rather than isolated facts, stay in your memory the night before the exam.
Head and neck anatomy decides more BDS results than any other region of the body, and the orbit, the pharyngeal apparatus, and the skull foramina sit right at the centre of that syllabus. Consequently, this guide condenses the most exam-relevant topics from BD Chaurasia’s Human Anatomy into one quick-revision article. Furthermore, every section below uses tables and a flowchart so that the relationships between structures, rather than isolated facts, stay in your memory the night before the exam.
osteology of head and neck The Orbit and Its Surrounding Structures
Orbit
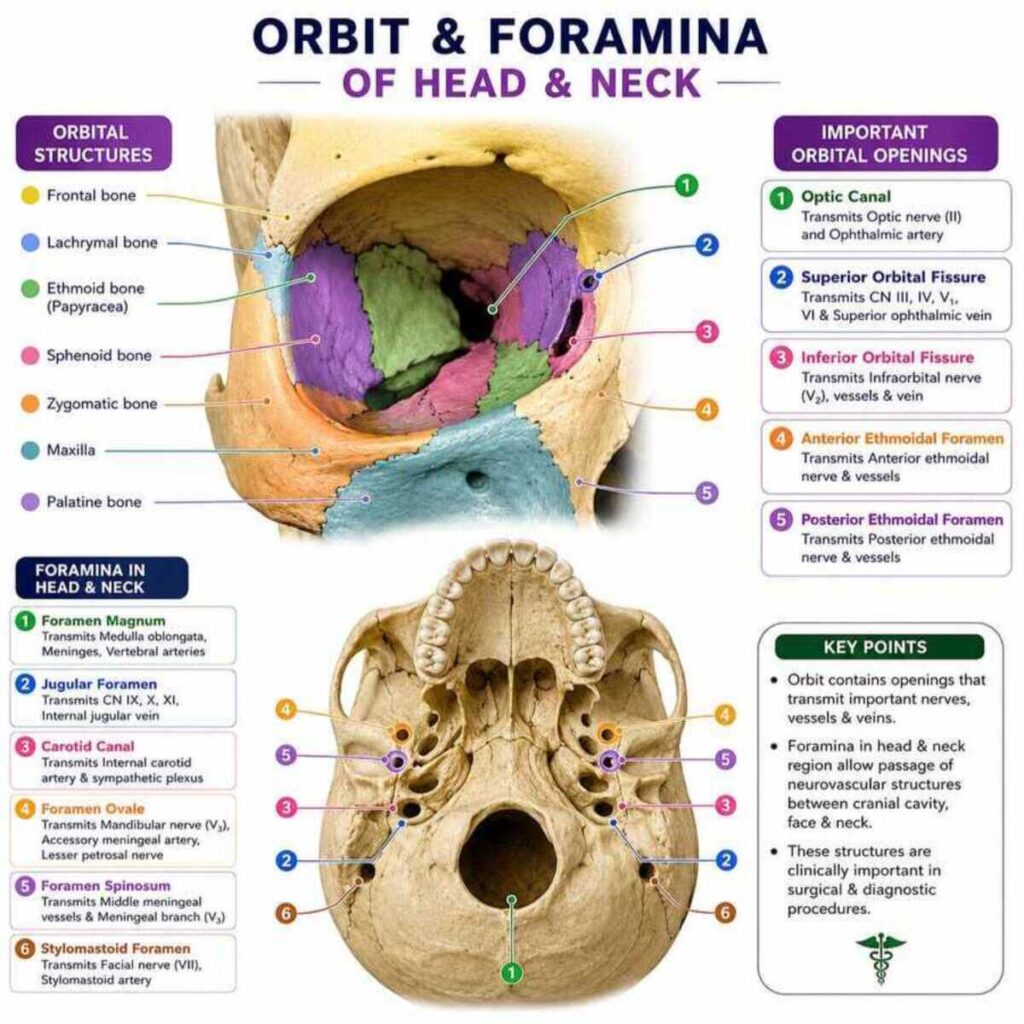
But the orbit is described as a pyramidal cavity whose base faces forward and whose apex points backward toward the optic canal. Thus, It is bounded by a roof, a floor, a medial wall, and a lateral wall, and each wall is formed by a predictable combination of bones. The roof, for instance, is formed mainly by the frontal bone, whereas the floor is formed by the maxilla, zygomatic bone, and palatine bone. Because the floor is also the roof of the maxillary sinus, a blow to the eye can fracture this thin plate and push orbital contents into the sinus below — a clinical scenario commonly tested as the “blow-out fracture.”
Foramina in Relation to the Orbit
Thus, osteology of head and neck Several openings communicate with the orbit, and examiners frequently ask which nerve or vessel passes through each one. But the table below organises this high-yield information for quick recall.
| Foramen/Fissure | Location | Main Structures Transmitted |
|---|---|---|
| Optic canal | Junction of roof and medial wall | Optic nerve, ophthalmic artery |
| Superior orbital fissure | Between roof and lateral wall | Oculomotor, trochlear, abducent, ophthalmic nerve |
| Inferior orbital fissure | Between floor and lateral wall | Maxillary nerve, zygomatic nerve, infraorbital vessels |
| Supraorbital notch/foramen | Superior margin | Supraorbital nerve and vessels |
| Anterior/posterior ethmoidal foramina | Medial wall | Ethmoidal nerves and vessels |
Eyelids and Palpebrae
The eyelids, also called palpebrae, protect the eyeball and spread the tear film with every blink. The upper eyelid additionally contains the levator palpebrae superioris, so damage to its nerve supply produces ptosis, a drooping lid that is a classic clinical sign. Meanwhile, the meibomian glands embedded in the tarsal plates secrete an oily layer that prevents the tear film from evaporating too quickly.
Lacrimal Apparatus
The lacrimal apparatus produces and drains tears, and it therefore includes the lacrimal gland, the lacrimal canaliculi, the lacrimal sac, and the nasolacrimal duct. Tears are first secreted by the lacrimal gland in the superolateral orbit; they then wash across the eye and enter the puncta before draining, via the canaliculi, into the lacrimal sac. From there, the nasolacrimal duct carries the fluid into the inferior nasal meatus, which explains why crying often causes a runny nose. In addition, inflammation of the lacrimal sac, known as dacryocystitis, is a frequently asked clinical correlation.
osteology of head and neck Facial Vasculature
Facial Artery
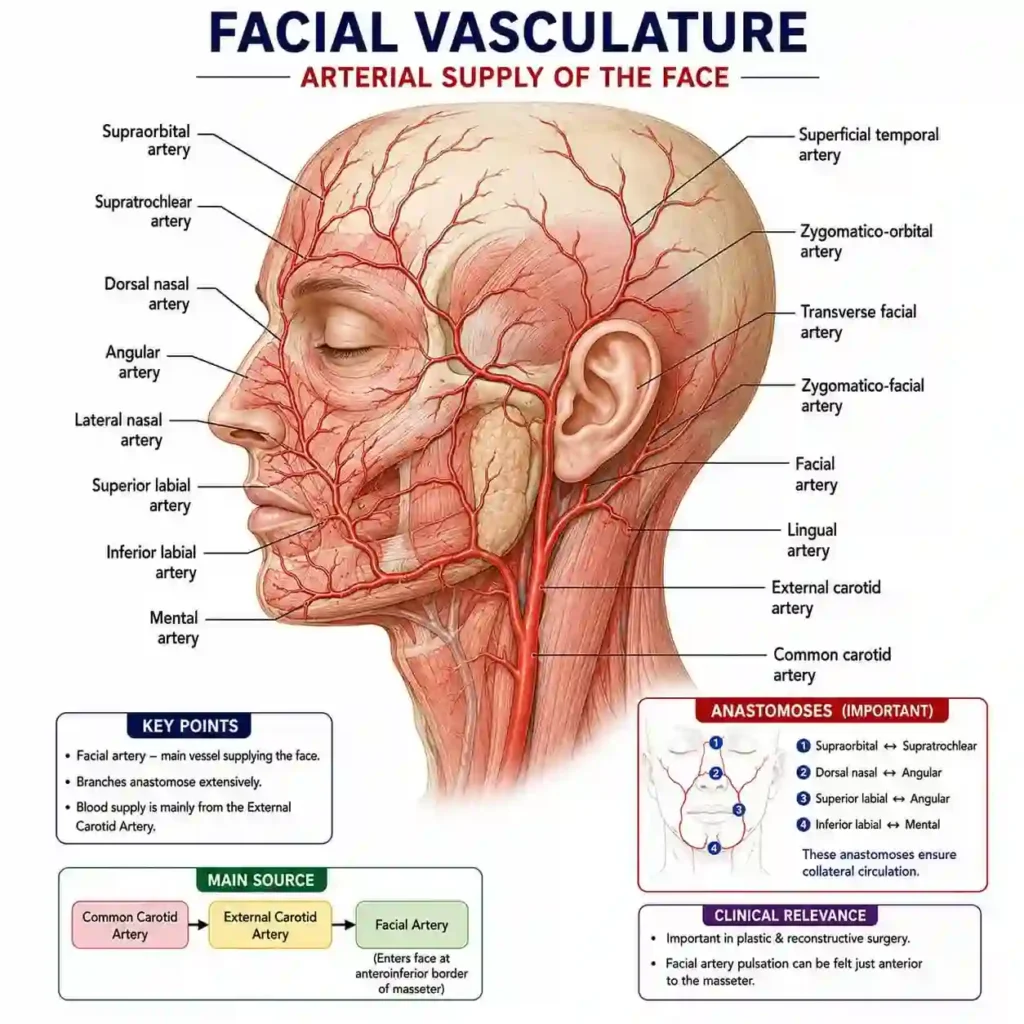
After arising in the carotid triangle, the artery passes deep to the submandibular gland, curls around the lower border of the mandible at the antero-inferior angle of the masseter, and then runs obliquely across the face toward the medial angle of the eye. Along this course, it gives off the inferior and superior labial branches, which supply the lips, as well as smaller branches to the submental and buccal regions. Because this artery is unusually tortuous, it can pulsate visibly, which is why clinicians use it as a reliable site to check the pulse in unconscious patients.
Development of the Skull
Ossification and Clinical Anatomy of the Maxilla and Maxillary Sinus
Thus, the maxilla ossifies in membrane from several centres that fuse around the developing tooth germs, and this membranous origin explains why maxillary fractures rarely involve true bone union problems the way long-bone fractures do. The maxillary sinus, meanwhile, begins as a shallow groove in the lateral nasal wall during foetal life and only reaches its full pyramidal size after the permanent teeth erupt. Clinically, this growth pattern matters a great deal in dentistry: the sinus floor lies extremely close to the roots of the premolars and molars, so periapical infection of these teeth can spread directly into the sinus. Therefore, dental students must correlate the anatomy with everyday clinical practice rather than memorising it in isolation.
Pharyngeal Apparatus and Its Derivatives
Mesodermal Derivatives of the Pharyngeal Arches
| Arch | Cartilage | Muscles | Nerve | Skeletal Derivative |
|---|---|---|---|---|
| 1st (Mandibular) | Meckel’s cartilage | Muscles of mastication, mylohyoid | Mandibular (V3) | Malleus, incus, mandible |
| 2nd (Hyoid) | Reichert’s cartilage | Muscles of facial expression | Facial (VII) | Stapes, styloid process, lesser cornu of hyoid |
| 3rd | Cartilage bar | Stylopharyngeus | Glossopharyngeal (IX) | Greater cornu and body of hyoid |
| 4th & 6th | Laryngeal cartilages | Pharyngeal constrictors, laryngeal muscles | Vagus (X) | Thyroid, cricoid, arytenoid cartilages |
Derivatives of the Pharyngeal (Ectodermal) Clefts and the Mandible
The mandible itself develops within the first arch around Meckel’s cartilage, which acts as a template rather than ossifying directly into bone; instead, membranous ossification occurs alongside the cartilage, and most of Meckel’s cartilage later degenerates while a small part contributes to the sphenomandibular ligament.
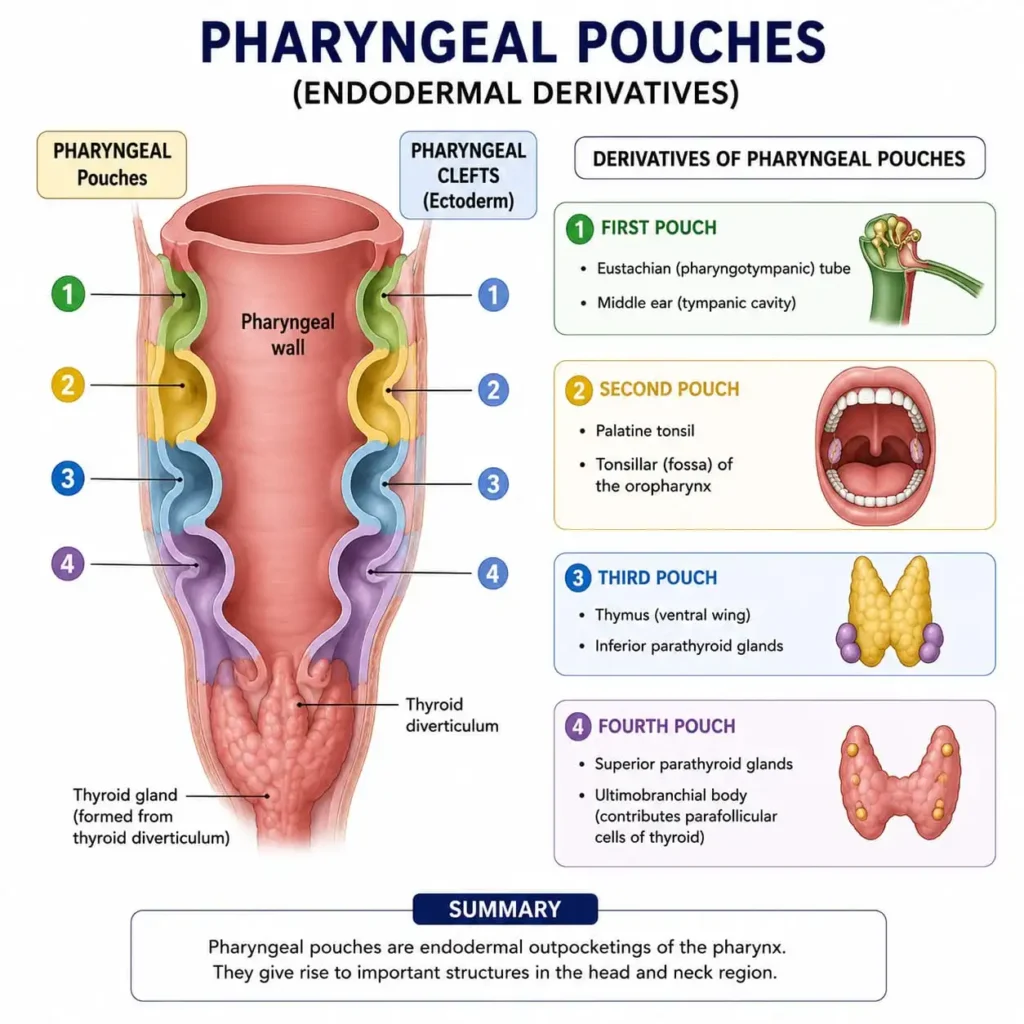
Derivatives of the Endodermal Pouches
The pharyngeal pouches, in contrast, line the inner surface of the pharynx and give rise to several important glands, as summarised below.
| Pouch | Major Derivative |
|---|---|
| 1st | Tympanic cavity, auditory tube |
| 2nd | Palatine tonsil |
| 3rd | Inferior parathyroid gland, thymus |
| 4th | Superior parathyroid gland |
Foramina in Relation to Nerves and Vessels
Because cranial foramina link gross anatomy with neuroanatomy, they remain one of the highest-yield revision areas overall. Thus, the table below lists the foramina most often asked in BDS examinations.
| Foramen | Structures Transmitted |
|---|---|
| Foramen rotundum | Maxillary nerve |
| Foramen ovale | Mandibular nerve, accessory meningeal artery |
| Foramen spinosum | Middle meningeal artery |
| Jugular foramen | Glossopharyngeal, vagus, accessory nerves; internal jugular vein |
| Stylomastoid foramen | Facial nerve |
| Foramen lacerum | Internal carotid artery (passes over, not through) |
Quick Embryology Flowchart
Pharyngeal Apparatus
|
├── Arches → Cartilage + Muscle + Nerve + Artery (mesoderm)
|
├── Clefts → External acoustic meatus (1st cleft only) + ectoderm
|
└── Pouches → Tympanic cavity, tonsil, parathyroids, thymus (endoderm)Final Revision Tips
In summary, the orbit, the facial artery, the foetal skull, and the pharyngeal apparatus are connected by one common thread: each topic links a developmental or anatomical fact to a real clinical scenario that dentists encounter routinely. Therefore, instead of memorising each topic in isolation, try drawing the tables and the flowchart above from memory, and then test yourself by tracing the facial artery’s course or naming each arch’s nerve aloud. With consistent, structured revision along these lines, these traditionally “high-weightage” BD Chaurasia topics become genuinely manageable rather than overwhelming.