The head and neck region is clinically important. Therefore, students usually study three regions together. These are the scalp, the temple, and the face. These regions share overlapping layers, vessels, and nerves. As a result, understanding them as one unit makes sense. The scalp blends into the temple. Similarly, the temple blends into the face. Consequently, trauma in one region can affect the others.
Surgeons often cross these boundaries during procedures. For example, facelifts and craniotomies are common cases. Therefore, knowledge of these transitions matters greatly. This guide explains each region in detail. In addition, it covers boundaries, layers, and blood supply. Furthermore, it explains the nerve supply of each area. Tables, a flowchart, and a concept map help. Moreover, clinical tidbits appear throughout the guide.
Textbooks often separate these three topics. However, you should picture them as one unit. Together, they form a continuous sheet of tissue. Therefore, this guide moves from scalp to face. It builds a complete picture step by step. As a result, you will learn sensation and circulation here.
Anatomy of the Scalp
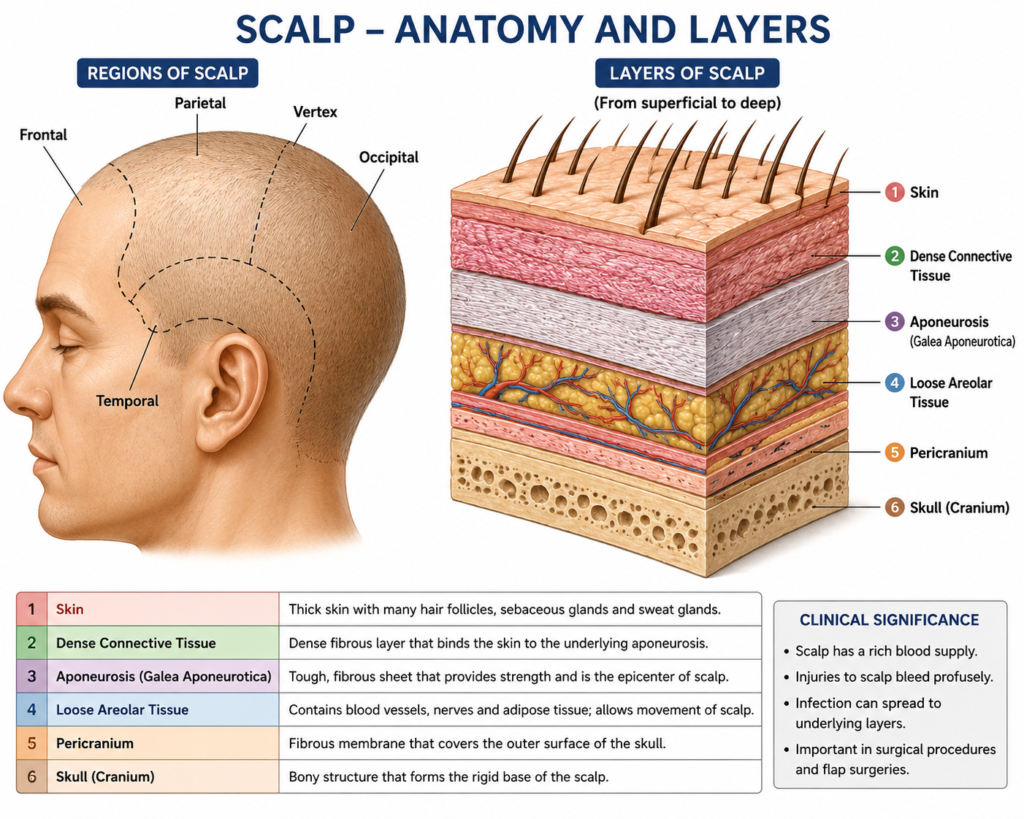
The scalp covers the head from front to back. It starts at the supraorbital margin. Then, it ends at the superior nuchal line. It also reaches the zygomatic arches on both sides. Because the scalp holds many vessels and nerves, cuts bleed heavily. Therefore, doctors apply firm pressure before suturing. The scalp follows a five-layer model. This layering explains both mobility and injury risk. For instance, newborns can get subgaleal hematomas here.
Students remember the scalp with “SCALP.” Each letter stands for one layer. These layers run from superficial to deep. As a result, learning them first helps a lot. Subsequently, blood and nerve supply become easier to learn. The connective tissue layer binds tightly to skin. It also binds to the muscle layer below. Therefore, this whole unit moves together as one. For example, raising your eyebrows shows this clearly.
The table below lists all five layers. It also shows their clinical importance.
| Layer | Name | Key Feature |
|---|---|---|
| S | Skin | Thick, hair-bearing, highly vascular |
| C | Connective tissue (dense) | Contains blood vessels and nerves |
| A | Aponeurosis (epicranial) | Connects frontalis and occipitalis muscles |
| L | Loose connective tissue | “Danger zone”; allows spread of infection |
| P | Pericranium | Periosteum of the skull bones |
Quick Tidbit: The loose connective tissue layer is the “danger zone.” Because infection spreads here, it can reach the brain. Consequently, it may cause meningitis.
Five major arteries supply the scalp. They arise from two carotid systems. The supratrochlear artery supplies the front. Similarly, the supraorbital artery supplies the front too. The superficial temporal artery supplies the side. Meanwhile, the occipital artery supplies the back area. These vessels connect freely with each other. Therefore, damage to one vessel is not fatal. As a result, other arteries keep blood flowing well.
The trigeminal nerve covers the front scalp. Meanwhile, cervical spinal nerves cover the back. Together, they cover the whole scalp fully. Therefore, no major gaps exist in coverage. For this reason, doctors target several nerves during a scalp block. Overall, the scalp is tough and resilient. Yet, it still bleeds heavily when cut.
Anatomy of the Temple
The temple sits beside the head. It lies between the orbit and ear. The temporal line marks its upper edge. Meanwhile, the zygomatic arch marks its lower edge. Unlike the scalp, skin here is thinner. Therefore, deeper layers sit closer to the surface. This includes the temporal fascia and muscle. As a result, surgeons must cut carefully here. The temple is also a useful landmark. For instance, you can feel the temporal artery here. Doctors check it for temporal arteritis.
Surgeons must know the fascial planes well. This matters during facelifts and brow lifts. It also matters during certain brain surgeries. Beneath these planes, the temporalis muscle sits. It fills the temporal fossa completely. Furthermore, it attaches to the mandible’s coronoid process. Consequently, damage here can weaken jaw closing. After all, the temporalis helps you chew food.
| Structure | Location | Clinical Relevance |
|---|---|---|
| Superficial temporal artery | Subcutaneous, anterior to ear | Palpated in temporal arteritis |
| Temporal fascia | Deep to subcutaneous tissue | Splits into two layers near zygomatic arch |
| Temporalis muscle | Temporal fossa | Elevates and retracts mandible |
| Auriculotemporal nerve | Posterior temple | Provides sensation; risk in facelift surgery |
Quick Tidbit: Surgeons stay above the deep temporal fascia. Because the facial nerve’s branch runs nearby, cutting too deep is risky.
Near the zygomatic arch, the fascia splits. It forms two separate layers there. In between, a small fat pad sits. Therefore, this detail matters greatly during surgery. If the wrong plane is cut, nerves get damaged. Consequently, this can cause forehead asymmetry. In the scalp, bleeding is the main risk. In contrast, nerve injury dominates here instead. For this reason, surgeons dissect this area very carefully.
Anatomy of the Face
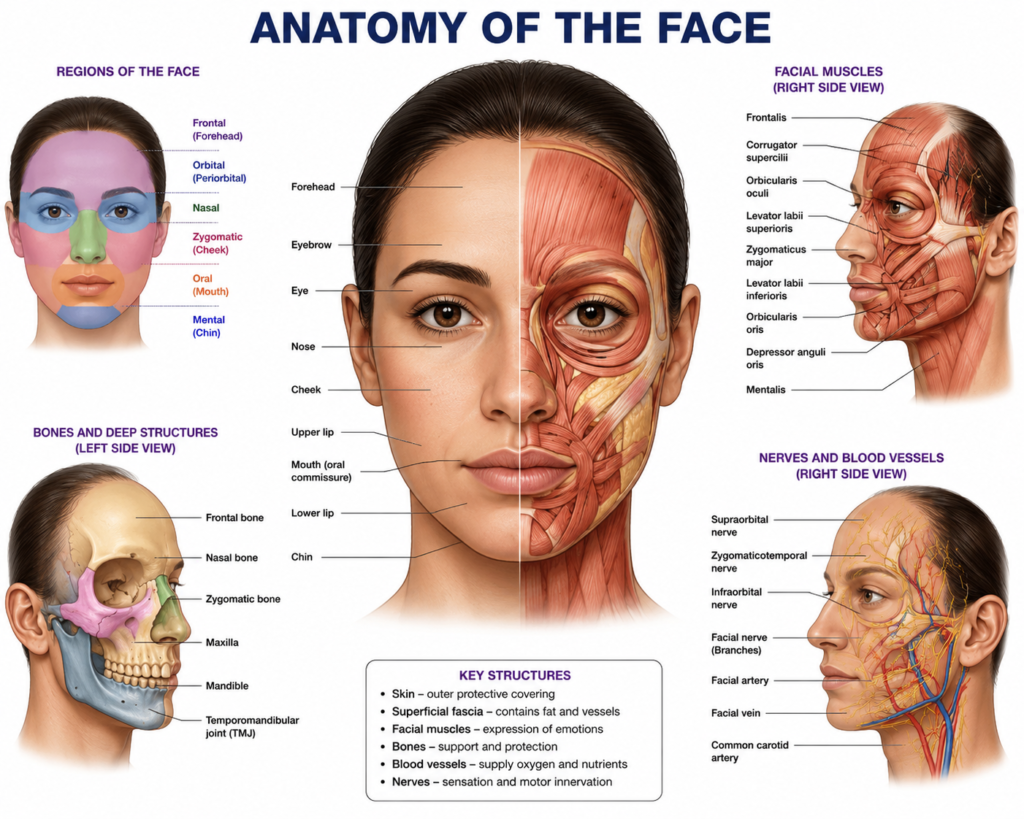
The face runs from the hairline to chin. It spans from one ear to the other. It is the most expressive body region. Because the facial nerve controls all expression, damage shows easily. For example, Bell’s palsy causes visible asymmetry. Facial skin is thinner than scalp skin. It is also far more mobile. As a result, this allows many subtle expressions.
Facial muscles group by their function. Some surround the eyes, nose, or mouth. Accordingly, a facial nerve branch controls each group. These branches exit the parotid gland first. Therefore, doctors use this to locate nerve damage. For instance, one-sided weakness suggests a lower lesion. In contrast, central lesions usually spare the forehead. The facial artery supplies most facial blood. In addition, the superficial temporal artery adds more. Likewise, the ophthalmic artery contributes some blood. Together, these vessels create strong redundancy.
| Facial Nerve Branch | Muscles Supplied | Common Clinical Test |
|---|---|---|
| Temporal | Frontalis, orbicularis oculi (upper) | Raise eyebrows |
| Zygomatic | Orbicularis oculi (lower) | Close eyes tightly |
| Buccal | Buccinator, orbicularis oris | Puff out cheeks |
| Marginal mandibular | Lower lip muscles | Show lower teeth |
| Cervical | Platysma | Tighten neck skin |
Simplified Flowchart: Facial Nerve Pathway
Facial Nerve (CN VII)
|
Exits Stylomastoid Foramen
|
Enters Parotid Gland
|
Branches Outward
/ | | \ \
Temporal Zygomatic Buccal Marginal CervicalQuick Tidbit: The facial nerve runs through the parotid gland. Therefore, parotid surgery risks nerve damage. This can affect the whole face.
The face needs three things working together. First, it needs muscle control from the facial nerve. Second, it needs sensation from the trigeminal nerve. Third, it needs a strong blood supply. Therefore, small problems here cause visible changes. Because the parotid gland sits close by, caution matters during surgery. In short, the face is a finely tuned system.
Concept Map: How the Three Regions Connect
SCALP
|
(shares vessels/nerves)
|
TEMPLE ---- (temporal fascia, facial nerve branch) ---- FACE
|
(zygomatic arch, hairline border)Overall, picture the scalp, temple, and face as one unit. They are not separate compartments. Because vessels and nerves cross between them, injuries spread easily. This holds true for both bleeding and nerve function. Therefore, learning this anatomy as a whole helps most. After all, it beats memorizing each part alone. In the end, this approach helps both study and practice.
Conclusion
The face, scalp, and temple are anatomically important regions of the head with complex structural organization. They contain vital bones, muscles, nerves, blood vessels, and fascial layers that work together to provide protection, movement, and sensation. The facial muscles are responsible for expression, speech, and mastication, while the scalp protects the skull and underlying brain.
The temple serves as an important anatomical landmark containing significant neurovascular structures. A sound understanding of the anatomy of these regions is essential for clinical examination and diagnosis. It also forms the basis for performing surgical procedures, administering local anesthesia, and managing facial injuries. Knowledge of these anatomical structures helps prevent complications during dental and maxillofacial treatment. Therefore, the anatomy of the face, scalp, and temple is fundamental for every dental and medical professional.
Frequently Asked Questions
The scalp follows the SCALP mnemonic. This stands for Skin, Connective tissue, Aponeurosis, Loose connective tissue, and Pericranium.
Because the temple lacks thick layers, nerves sit closer to the surface. Therefore, injury risk rises during surgery.
The facial nerve, or cranial nerve VII, controls it. Accordingly, it supplies every muscle of expression.
Blood vessels and nerves cross between all three. Therefore, they function as one continuous unit.