The neck connects the head to the trunk, and it houses vital structures within a small space. Surgeons, radiologists, and students study this region closely because it contains nerves, vessels, and muscles in tight arrangement. Therefore, understanding surface landmarks and fascial layers helps clinicians plan safe procedures.
This guide covers the major landmarks, the layers of deep cervical fascia, the posterior triangle, and the sternocleidomastoid muscle. Each section uses simple language and short sentences for easy reading. Tables and a flowchart break down complex relationships, so the content stays clear and practical for learners at every level.
Landmarks on the Side of the Neck
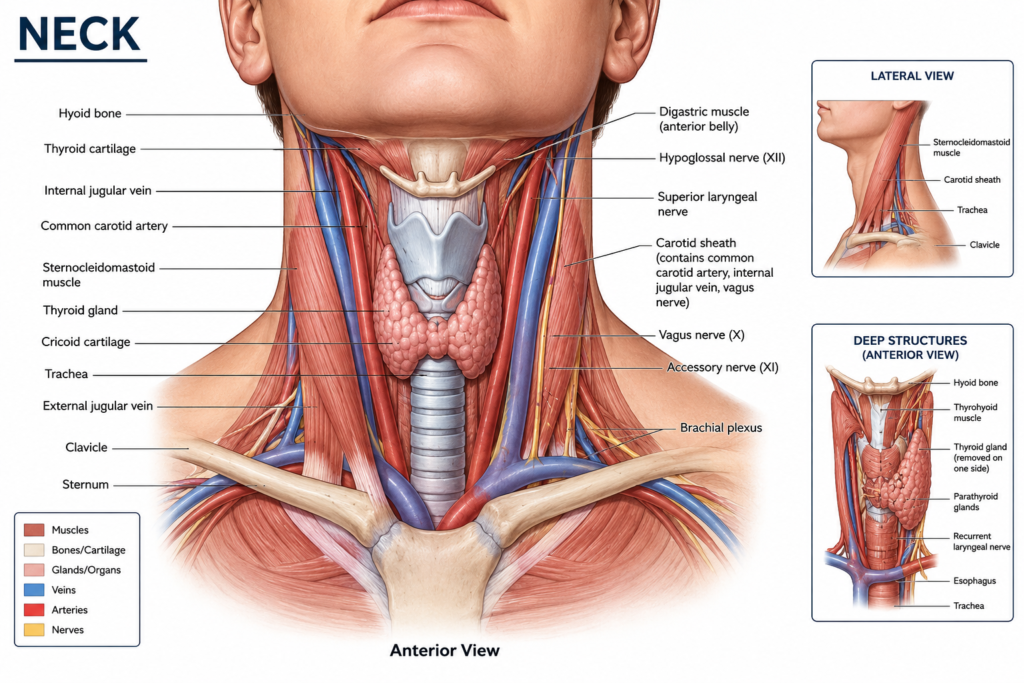
Surface landmarks act as reference points for clinical examination and surgical access. Palpation of these points allows doctors to locate deeper structures without imaging. Consequently, anatomy students memorize these landmarks early in their training.
The table below lists the key landmarks found on the lateral aspect of this region.
| Landmark | Location | Clinical Importance |
|---|---|---|
| Mastoid process | Behind the ear | Attachment site for sternocleidomastoid |
| Hyoid bone | Midline, level of C3 | Reference for laryngeal structures |
| Thyroid cartilage | Below the hyoid | Marks the larynx |
| Cricoid cartilage | Below thyroid cartilage | Site for emergency airway access |
| Clavicle | Base of the region | Lower boundary marker |
In addition, the anterior and posterior borders of the sternocleidomastoid muscle divide the area into anterior and posterior triangles. As a result, clinicians use these borders to describe the exact location of swellings, masses, or injuries during examination.
Deep Cervical Fascia: An Overview
The deep cervical fascia forms a supportive sheath around muscles, vessels, and organs in this region. It differs from the superficial fascia, which lies just beneath the skin. Unlike superficial fascia, the deep layer contains tough connective tissue that compartmentalizes structures effectively.
This fascial system splits into several distinct layers. Each layer wraps specific structures and creates potential spaces that can guide the spread of infection. For instance, dental infections can travel along fascial planes toward the chest if left untreated. Hence, surgeons study these layers carefully before performing neck procedures.
Layers of the Deep Cervical Fascia
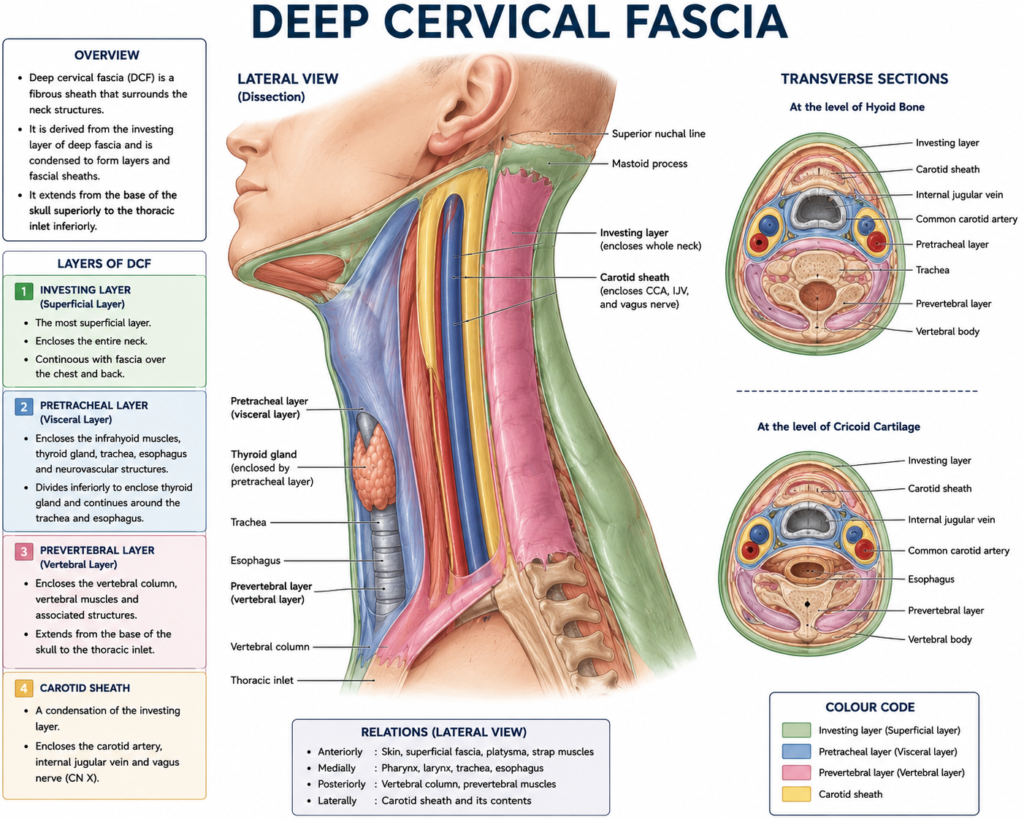
Three primary layers make up the deep cervical fascia, and each layer serves a unique purpose.
Investing Layer
The investing layer forms the outermost layer of deep fascia. It encircles the entire region like a collar and splits to enclose the sternocleidomastoid and trapezius muscles. Moreover, this layer attaches to the mandible above and the clavicle below.
Pretracheal Layer
The pretracheal layer lies anterior to the trachea and esophagus. It encloses the thyroid gland, trachea, and esophagus within a single fascial compartment. Similarly, this layer extends laterally to blend with the carotid sheath on both sides.
Prevertebral Layer
The prevertebral layer covers the vertebral column and the muscles attached to it. It lies posterior to the pharynx and esophagus, forming a tough barrier. Notably, this layer creates a potential space that can allow infection to spread toward the posterior mediastinum.
The table below summarizes these three layers for quick comparison.
| Fascial Layer | Position | Structures Enclosed |
|---|---|---|
| Investing layer | Outermost | Sternocleidomastoid, trapezius |
| Pretracheal layer | Anterior compartment | Thyroid, trachea, esophagus |
| Prevertebral layer | Posterior compartment | Vertebral column, deep muscles |
The Carotid Sheath
The carotid sheath forms a tubular fascial covering around major vessels and a nerve. It contains the common carotid artery, internal jugular vein, and vagus nerve. Additionally, this sheath receives contributions from all three layers of deep fascia described above.
The carotid sheath runs from the base of the skull to the root of this region. Surgeons identify it during procedures such as carotid endarterectomy or central line placement. Because the vagus nerve travels within this sheath, careful dissection prevents nerve damage during surgery.
Buccopharyngeal and Pharyngobasilar Fascia
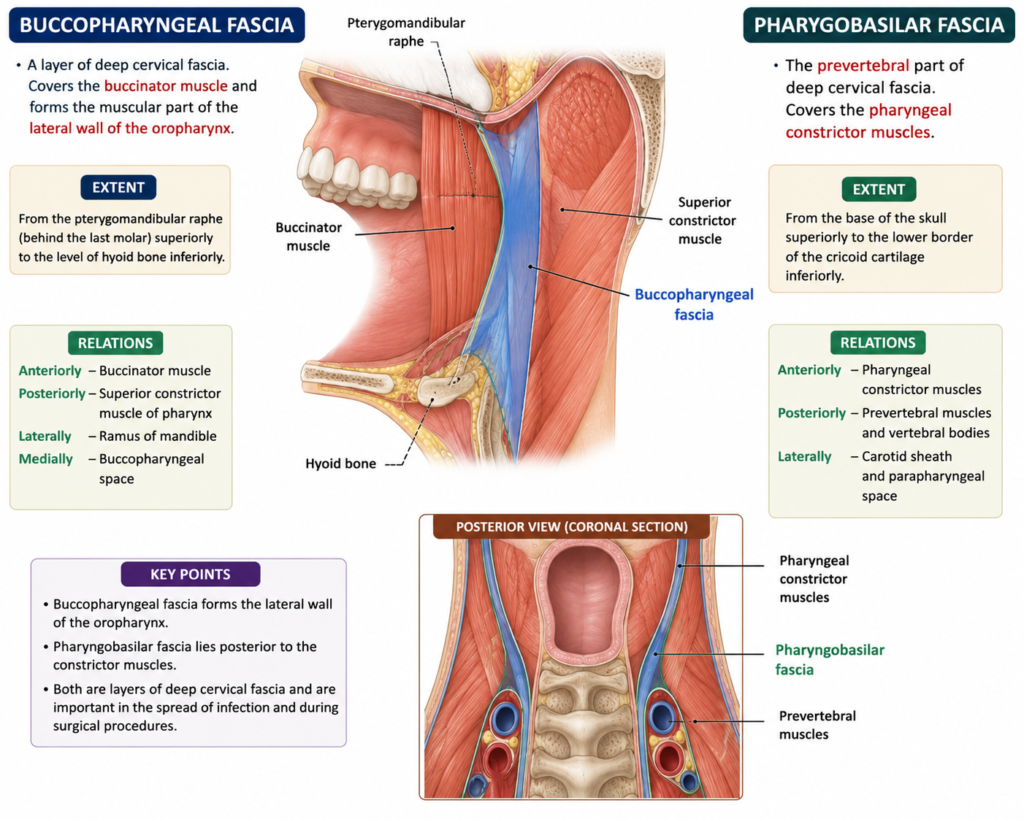
The buccopharyngeal fascia covers the outer surface of the pharyngeal constrictor muscles. It continues forward over the buccinator muscle inside the cheek. This fascia provides a smooth surface that allows the pharynx to move during swallowing.
In contrast, the pharyngobasilar fascia lies on the inner aspect of the pharynx, between the mucosa and the muscular wall. It attaches firmly to the base of the skull, hence its name. This fascia strengthens the upper pharynx, particularly where muscle fibers are thin or absent.
Both fascial sheets work together to support pharyngeal function. The buccopharyngeal layer protects the outside, while the pharyngobasilar layer reinforces the inside. Together, they maintain the structural integrity of the pharynx during breathing and swallowing.
The Posterior Triangle
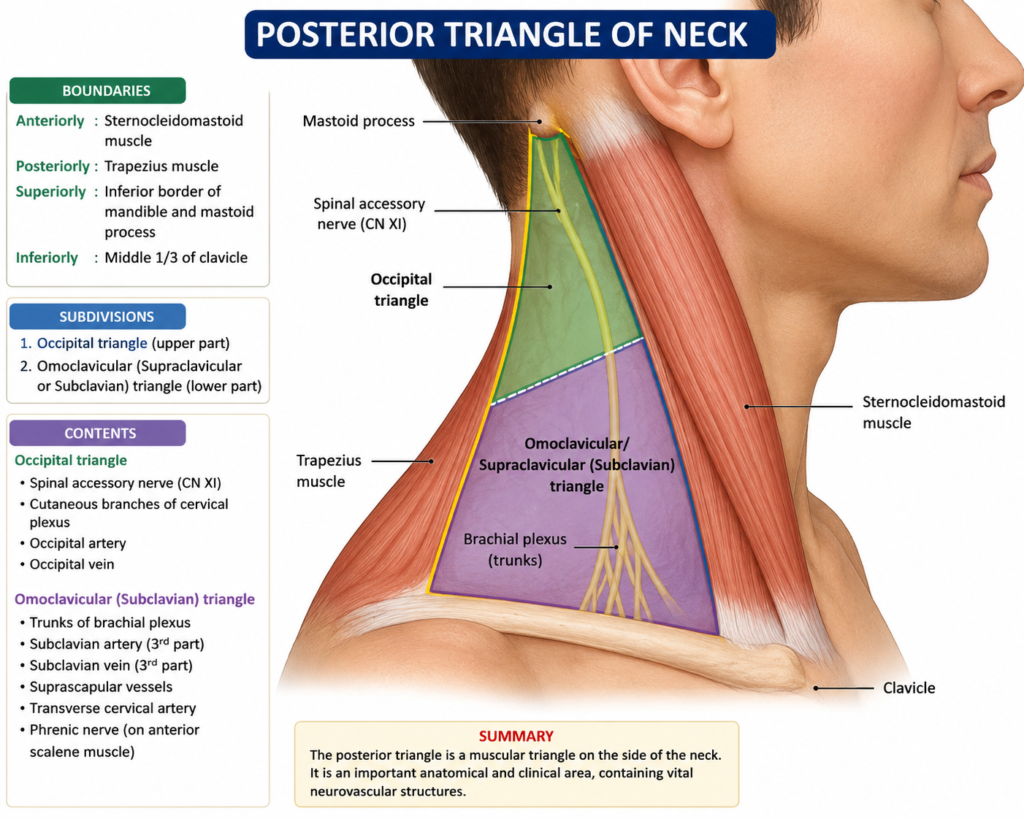
The posterior triangle occupies the area behind the sternocleidomastoid muscle. The trapezius muscle forms its posterior border, and the clavicle forms its base. This triangle contains important nerves and vessels that travel toward the upper limb and shoulder.
The flowchart below outlines the boundaries of this triangle in a simple sequence.
Sternocleidomastoid (anterior border)
|
v
Posterior Triangle Boundaries
|
------------------
| | |
Trapezius Clavicle Apex
(posterior) (base) (occipital bone)Several structures cross this triangle, including the accessory nerve, the brachial plexus trunks, and the subclavian artery. Therefore, surgeons approach this triangle cautiously to avoid nerve injury. Lymph nodes also collect in this space, so clinicians examine it during cancer staging.
Sternocleidomastoid Muscle
The sternocleidomastoid muscle stands as the most prominent muscle in this region. It originates from the sternum and clavicle, then inserts onto the mastoid process. This muscle divides the lateral region into the anterior and posterior triangles, making it a key surgical landmark.
Functionally, the sternocleidomastoid rotates the head to the opposite side when one side contracts. When both sides contract together, the muscle flexes the head forward. Consequently, physiotherapists assess this muscle when evaluating torticollis or whiplash injuries.
The spinal accessory nerve supplies this muscle and travels through it before entering the posterior triangle. Surgeons must identify this nerve during lymph node biopsies near this muscle. Otherwise, accidental injury can cause shoulder weakness and pain.
Quick Reference Summary
| Structure | Key Feature |
|---|---|
| Landmarks | Mastoid process, hyoid, thyroid cartilage, clavicle |
| Investing fascia | Encloses sternocleidomastoid and trapezius |
| Pretracheal fascia | Encloses thyroid, trachea, esophagus |
| Prevertebral fascia | Covers vertebral column |
| Carotid sheath | Contains artery, vein, and vagus nerve |
| Posterior triangle | Bounded by trapezius, clavicle, sternocleidomastoid |
Conclusion
The side of the neck contains a compact arrangement of muscles, vessels, and fascial layers. Each layer of deep cervical fascia serves a distinct protective role, while the carotid sheath safeguards major vessels and a nerve. Meanwhile, the posterior triangle and the sternocleidomastoid muscle act as practical guides for clinical examination. Together, these structures form a well-organized system that supports movement, swallowing, and protection of vital pathways.
Frequently Asked Questions
The sternocleidomastoid muscle is the main muscle on the side of the neck. It divides the region into anterior and posterior triangles.
The carotid sheath contains the common carotid artery, the internal jugular vein, and the vagus nerve.
The deep cervical fascia has three main layers: the investing layer, the pretracheal layer, and the prevertebral layer.
The sternocleidomastoid muscle forms the anterior border, the trapezius forms the posterior border, and the clavicle forms the base.
The pharyngobasilar fascia strengthens the upper pharynx and attaches firmly to the base of the skull, supporting swallowing function.