The orbit is a bony cavity that protects the eyeball and supports several vital structures. For dental and maxillofacial professionals, this region matters greatly. Many oral and facial procedures sit close to the orbital floor. Therefore, understanding the contents of orbit helps clinicians avoid serious complications during surgery.
This guide explains the major nerves, arteries, and muscles inside the orbit. Additionally, it includes simple tables and flowcharts for quick revision. Let’s explore this fascinating anatomical region step by step.
What Are the Contents of Orbit?
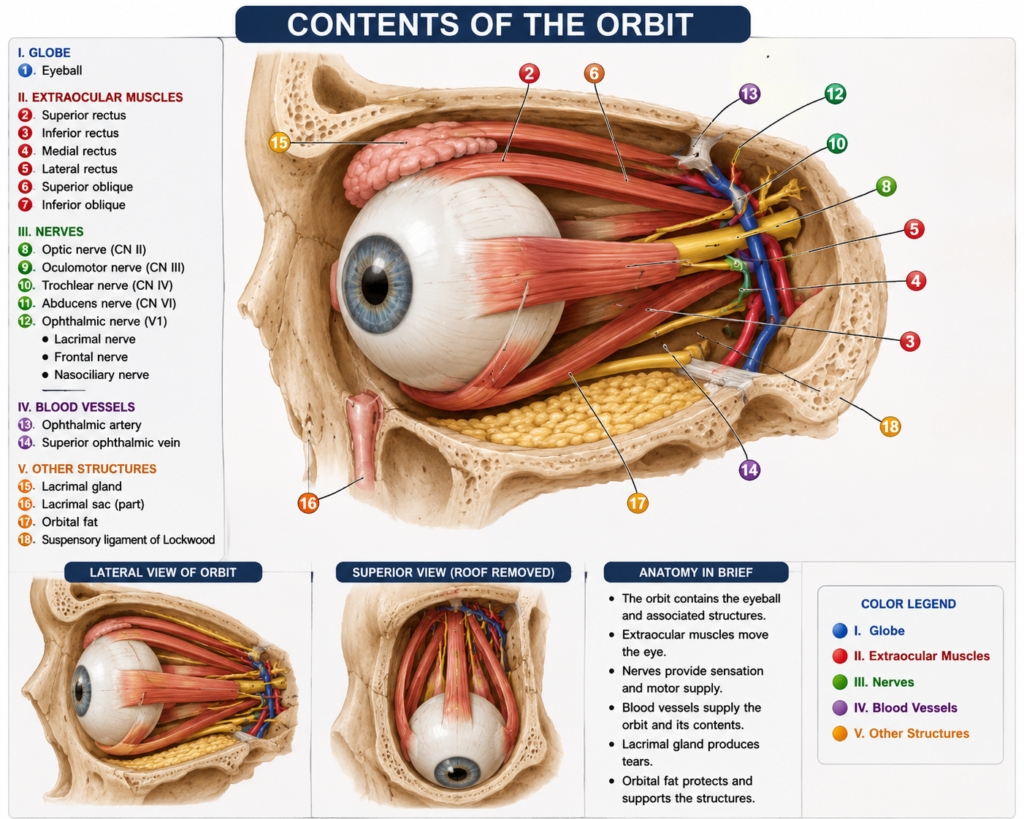
Before diving into details, it helps to see the full picture. The contents of orbit include muscles, nerves, vessels, fat, and connective tissue. Each structure plays a unique role in eye movement, sensation, or blood supply.
Below is a quick summary table.
| Structure | Type | Main Function |
|---|---|---|
| Extraocular muscles | Muscle | Eye movement |
| Ophthalmic artery | Artery | Blood supply to eye and orbit |
| Ophthalmic nerve | Sensory nerve | Sensation to forehead, eye, nose |
| Oculomotor nerve | Motor nerve | Controls most eye muscles |
| Trochlear nerve | Motor nerve | Supplies superior oblique muscle |
| Abducens nerve | Motor nerve | Supplies lateral rectus muscle |
| Ciliary ganglion | Parasympathetic ganglion | Controls pupil and lens |
Now, let’s examine each structure individually.
Extraocular Muscles
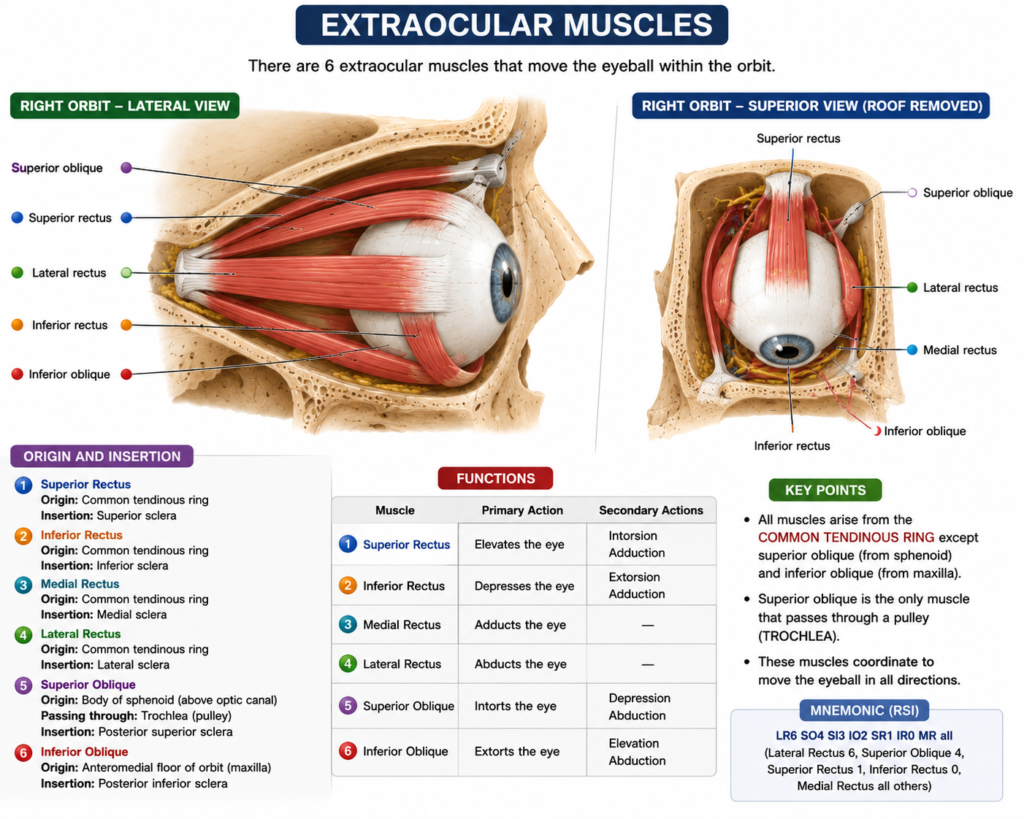
Seven muscles control eye movement and eyelid position. Six of these are true extraocular muscles, while one controls the upper eyelid.
The muscles include:
- Superior rectus
- Inferior rectus
- Medial rectus
- Lateral rectus
- Superior oblique
- Inferior oblique
- Levator palpebrae superioris
Most of these muscles arise from a common tendinous ring called the annulus of Zinn. Consequently, this ring acts as a central anchor point near the orbital apex. Meanwhile, the superior oblique and levator palpebrae superioris attach slightly differently, giving them unique movement patterns.
Interestingly, three separate nerves supply these seven muscles. As a result, damage to any single nerve produces a distinct and predictable pattern of eye movement loss. This fact makes neurological examination of eye movements clinically valuable.
Ophthalmic Artery and Nerve
The ophthalmic artery is the first major branch of the internal carotid artery after it exits the cavernous sinus. It enters the orbit through the optic canal, traveling alongside the optic nerve.
This artery supplies blood to several important areas. For instance, it nourishes the eyeball, extraocular muscles, eyelids, and parts of the nose and forehead. Furthermore, it gives rise to the central retinal artery, which supplies the retina directly. Blockage of this small branch can cause sudden, painless vision loss.
The ophthalmic nerve, on the other hand, is purely sensory. It represents the first division of the trigeminal nerve (CN V1). It enters the orbit through the superior orbital fissure and divides into three branches: frontal, lacrimal, and nasociliary.
Because the ophthalmic nerve carries sensation from the eye, forehead, and upper nose, dental professionals should recognize its pathways. Occasionally, facial pain conditions overlap with trigeminal branches, so accurate localization matters.
Oculomotor Nerve (CN III)
The oculomotor nerve is the major motor nerve of the orbit. It supplies four of the six extraocular muscles: superior rectus, inferior rectus, medial rectus, and inferior oblique. Additionally, it supplies the levator palpebrae superioris.
This nerve also carries parasympathetic fibers. These fibers travel to the ciliary ganglion and control pupil constriction along with lens accommodation.
Clinically, oculomotor nerve palsy causes a classic presentation. The eye deviates downward and outward, the eyelid droops, and the pupil may become dilated. Therefore, this nerve holds high diagnostic value in cranial nerve examinations.
Ciliary Ganglion
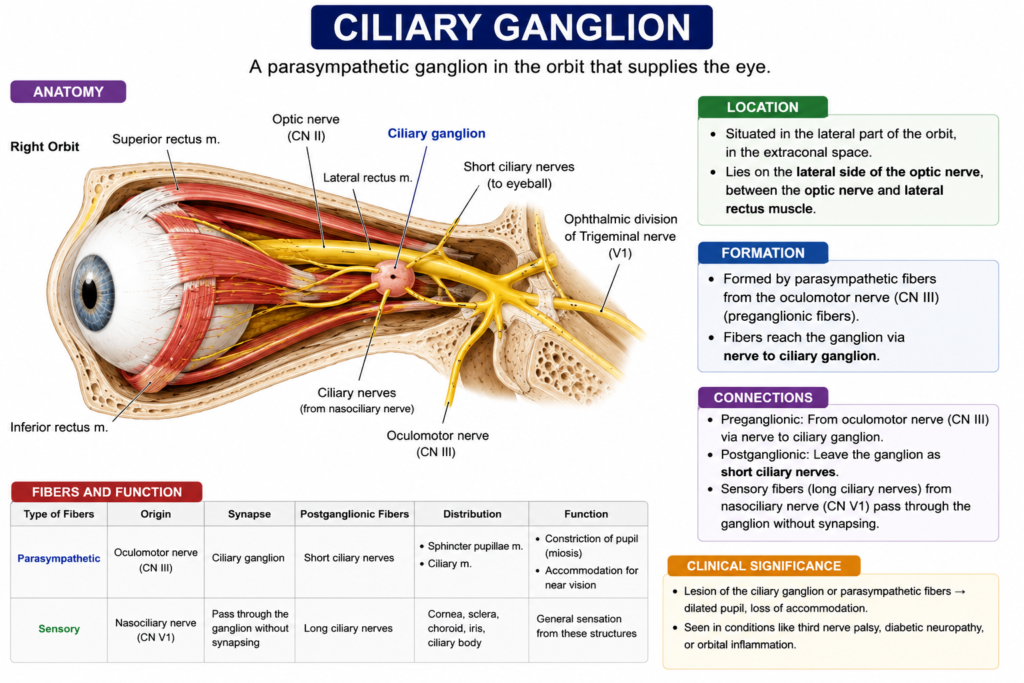
The ciliary ganglion is a small parasympathetic ganglion located within the orbit. It sits near the optic nerve, close to the apex of the orbit.
Three types of nerve fibers pass through or relate to this ganglion:
- Parasympathetic fibers from the oculomotor nerve, which synapse here
- Sympathetic fibers, which pass through without synapsing
- Sensory fibers from the nasociliary nerve, which also pass through
After synapsing, postganglionic parasympathetic fibers leave as short ciliary nerves. These nerves then supply the ciliary muscle and the sphincter pupillae. Subsequently, this pathway allows pupil constriction and lens shape changes during near vision.
Below is a simple flowchart showing this pathway.
Oculomotor Nerve (CN III)
|
v
Ciliary Ganglion (synapse)
|
v
Short Ciliary Nerves
|
v
Sphincter Pupillae + Ciliary MuscleTrochlear Nerve and Artery
The trochlear nerve (CN IV) supplies only one muscle: the superior oblique. Despite this limited role, it holds an interesting distinction. It is the only cranial nerve that exits from the back of the brainstem. It is also the thinnest cranial nerve overall.
This nerve enters the orbit through the superior orbital fissure, outside the annulus of Zinn. Then, it travels above the levator palpebrae superioris to reach the superior oblique muscle.
Regarding the trochlear artery, no single dedicated vessel carries this exact name in standard anatomy texts. Instead, small branches from the ophthalmic artery supply the superior oblique muscle and surrounding tissue. These branches travel alongside the trochlear nerve pathway, supporting the same regional structures.
Damage to the trochlear nerve causes vertical diplopia, especially while looking downward. Patients often notice this problem when reading or walking down stairs.
Abducens Nerve and Artery
The abducens nerve (CN VI) supplies the lateral rectus muscle. This muscle abducts the eye, moving it laterally away from the nose.
This nerve has a long intracranial course. It travels through the cavernous sinus before entering the orbit through the superior orbital fissure. Because of this long path, the abducens nerve is particularly vulnerable to compression from raised intracranial pressure.
Similar to the trochlear artery, the abducens artery is not a distinct named vessel. Instead, small branches from the ophthalmic artery and its muscular branches supply the lateral rectus muscle and nearby abducens nerve pathway.
Abducens nerve palsy produces a classic sign. The affected eye cannot move outward, causing the eye to drift inward at rest. Patients typically report horizontal double vision.
Quick Comparison of Orbital Nerves
| Nerve | Number | Muscle Supplied | Type |
|---|---|---|---|
| Oculomotor | CN III | SR, IR, MR, IO, LPS | Motor + Parasympathetic |
| Trochlear | CN IV | Superior oblique | Motor |
| Abducens | CN VI | Lateral rectus | Motor |
| Ophthalmic | CN V1 | None (sensory only) | Sensory |
Why This Matters for Dental Professionals
Many maxillofacial procedures occur close to the orbital floor and infraorbital region. For example, zygomatic implant placement and orbital floor fracture repair both demand precise anatomical knowledge. Likewise, sinus lift procedures sometimes approach areas near orbital structures.
Therefore, dentists and oral surgeons benefit greatly from reviewing the contents of orbit regularly. This knowledge helps prevent nerve injury, vascular damage, and postoperative visual complications.
Conclusion
The contents of orbit form a complex but logical system. Muscles control movement, nerves provide sensation and motor function, and arteries supply essential nutrients. Understanding the contents of orbit allows dental and medical professionals to work safely near this delicate region.
Moreover, recognizing nerve palsies and their clinical signs supports faster, more accurate diagnosis. Whether you are a dental student or a practicing clinician, mastering this anatomy builds confidence during facial and maxillofacial procedures. Ultimately, this knowledge protects patient safety and improves surgical outcomes.
Frequently Asked Questions
The contents of orbit include extraocular muscles, the ophthalmic artery and nerve, the oculomotor, trochlear, and abducens nerves, the ciliary ganglion, fat, and connective tissue.
The oculomotor nerve supplies the most muscles. It controls the superior rectus, inferior rectus, medial rectus, inferior oblique, and the levator palpebrae superioris.
The ciliary ganglion relays parasympathetic fibers from the oculomotor nerve. These fibers control pupil constriction and lens accommodation through short ciliary nerves.
The trochlear nerve is the only cranial nerve that exits from the back of the brainstem. It is also the thinnest cranial nerve in the body.
Damage to the abducens nerve weakens the lateral rectus muscle. This causes the eye to drift inward and produces horizontal double vision.